This is Part 3 of 3 in the Hair Series. The full path:
- Part 1 - The Diagnostic (2 sub-articles):
- Part 1.1: What Actually Matters?
- Part 1.2: How to Actually Track and Decide
- Part 2 (this article): The Stack and the Routine - the pharmacology and the daily layered schedule
Important framing This article splits the stack into two tiers — Tier 1 (compounds with legal sourcing routes through clinics and pharmacies in Malaysia) and Tier 2 (research compounds sourced through grey-market channels, with real risk profiles and minimal long-term human safety data).
The first tier is appropriate for almost anyone serious about treating androgenetic alopecia. The second tier is not a recommendation — it’s a transparency layer on what exists in the broader protocol space. Both tiers assume the diagnostic groundwork from Part 1.1 and Part 1.2 is already done.
Nothing here is medical advice. Bloodwork and a physician familiar with what’s being run are non-negotiable for anything in Tier 2.
Table of Contents
- Bridge from Part 1.2
- The 90/10 frame
- The deliberate exclusion: why no finasteride or dutasteride
- Tier 1 — The Pharmacy Stack
- Tier 2 — The Research Stack
- Beyond pharmacology — mechanical and environmental protocols
- Sourcing tiers
- Bloodwork
- The optimized daily and weekly schedule
- Layering rules
- Cycle management
- How to think about all of this
- Part 2.0 Takeaways
- Your Tier-1 Stack Task List
- Sources & references
Bridge from Part 1.2
Part 1.1 established what’s biologically possible and what the three diagnostic KPIs measure. Part 1.2 anchored the baseline, set the 12-month timeline, and built the attribution map showing which compound in the stack drives which KPI.
This article is the stack itself: what each compound is, what it does, what dose runs it, where it’s sourced, and how the whole thing layers into a daily schedule that doesn’t fight itself. Then the closing piece — why we deliberately don’t run the two most famous AGA drugs in the world (finasteride and dutasteride).
The 90/10 frame
Same framing as the Fit Series Part 4.0 for supplements.
- 90% of the result comes from the diagnostic loop and basic consistency — anchoring the baseline at a clinic, hitting the protocol every day, holding through the Month-3 dread shed, re-evaluating at Month 6 and Month 12. Skipping doses for two weeks because life got busy costs more than picking the wrong compound.
- The other 10% is the chemistry — which receptors are blocked, which channels are opened, which growth signals are firing. This article is the 10%. It is meaningful, but only after the 90% is locked in.
People run this backward. They obsess over RU58841 vehicle ratios while applying minoxidil three nights a week. The compound choice doesn’t matter if the schedule doesn’t hold.
The deliberate exclusion: why no finasteride or dutasteride
The most well-studied, FDA-approved, decades-of-data drugs for AGA are finasteride and dutasteride — both 5α-reductase inhibitors (5αRI). They work by stopping testosterone from converting to DHT, which removes the upstream signal for follicular miniaturization. They’re effective. And they are deliberately not in this stack.
Two reasons stack, and either one alone would be sufficient.
Reason 1: Mechanism conflict with DHT-derivative use
When the broader hormonal protocol includes exogenous androgens or DHT-derived compounds, systemic 5α-reductase inhibition either doesn’t help (DHT-derivatives bypass 5αR entirely — they’re already past that step in the pathway) or creates direct conflict with the rest of the protocol. The 5αRI has nothing useful to block in that context.
Reason 2: Allopregnanolone reduction and the motivation cost
5α-reductase doesn’t only convert testosterone to DHT. It also converts progesterone to allopregnanolone, a potent positive allosteric modulator of the GABA-A receptor.1 Allopregnanolone is one of the brain’s primary endogenous anxiolytics and is involved in mood regulation, stress resilience, motivation, and libido.
When 5αRI is given systemically, allopregnanolone production drops alongside DHT. For a meaningful fraction of users, this produces well-documented downstream effects — low mood, anhedonia, anxiety, low libido, brain fog — collectively referred to as post-finasteride syndrome (PFS) when persistent.2 Not everyone is sensitive, but the protocol stance is straightforward: if mood, drive, and clarity are load-bearing for everything else (work, training, life), the trade isn’t worth it when localized alternatives exist.
What replaces it: localized androgen receptor blockade
RU58841 is the substitute. It’s an androgen receptor antagonist — it binds the receptor in scalp follicles and prevents DHT from binding, achieving the same downstream effect (no miniaturization signal) without touching 5α-reductase systemically. Applied topically, the effect stays largely local to the scalp. Allopregnanolone production is preserved. DHT-derivative protocols continue unaffected.
The trade-off: RU58841 is grey-market, has no completed long-term human safety trials, and requires daily topical adherence forever. Finasteride is one pill a day with decades of safety data. The choice is mood preservation and protocol compatibility vs. proven convenience.
Not a universal recommendation For someone who isn't running androgens and isn't sensitive to 5αRI side effects, finasteride is still the most evidence-backed AGA drug on earth and a perfectly reasonable Tier-1 choice. The deliberate exclusion in this stack is a context-specific decision, not a general claim that finasteride is bad.
Tier 1 — The Pharmacy Stack
Compounds with legal sourcing routes through Malaysian clinics and pharmacies (with prescription). Mechanism → use case → dose → downsides for each.
Oral minoxidil
A potassium-channel opener originally developed as an oral antihypertensive. Off-label use at low doses for AGA has become the standard-of-care alternative to topical minoxidil over the past 5 years — better adherence (one pill vs. a daily scalp ritual), better systemic delivery, and dose-dependent density gains.3
Mechanism. Opens potassium channels in vascular smooth muscle → vasodilation around the follicle → increased blood flow, oxygen, and nutrient delivery → dormant follicles re-enter anagen and existing follicles expand.
Dose ranges and what they do:
| Daily dose | Use case | Expected response window |
|---|---|---|
| 0.625–1.25 mg | Mild diffuse thinning or initial trial; minimize cardiovascular side effects | Low; mostly maintenance |
| 2.5 mg | The mainstream sweet spot for most natural lifters with active AGA | Meaningful density gains by Month 6 |
| 5 mg | More aggressive cases, established miniaturization, when 2.5 mg plateaus | Stronger response, higher side-effect probability |
| >5 mg | Rarely necessary for hair use; pure dose-response curve flattens | Diminishing returns, higher cardiovascular load |
The 2.5–5 mg range is the operating window for this protocol. Most people do well starting at 2.5 mg and titrating up to 5 mg only if the Month-6 audit shows a density gap in Part 1.2’s Branch 1 (T:V improving, density flat).
Downsides. Mild fluid retention, occasional ankle swelling, modest resting heart rate increase, possible body hair growth (a feature for some, a bug for others). At the 2.5–5 mg range these are usually manageable; above 5 mg they become more reliable. Cardiovascular history (hypertension, arrhythmia) is a contraindication.
Topical minoxidil + tretinoin
The combination that turns the topical minoxidil layer from “okay” into the actual driver of follicular density at the regional level.
Mechanism. Topical minoxidil delivers the vasodilation effect directly to the application zone. The catch: minoxidil is a prodrug — it has to be converted to minoxidil sulfate by the scalp enzyme sulfotransferase (SULT1A1) before it’s bioactive. A meaningful fraction of the population are “non-responders” or “weak responders” because their scalp SULT1A1 activity is low.4
Tretinoin (a topical retinoid) upregulates SULT1A1, converting non-responders into responders and amplifying response in everyone else. The combination is more effective than minoxidil alone in essentially every published comparison.
Doses.
- Topical minoxidil: 5% — the operating concentration. Lower (2%) is the Rogaine-women’s-version and underdoses the scalp. Higher (7%, 10%, 15%) increases scalp irritation faster than it increases response — diminishing returns above 5%.
- Tretinoin: 0.025% — the operating concentration for combined use. The higher dermatology doses (0.05%, 0.1%) are for facial acne and produce too much scalp irritation when layered with minoxidil. 0.025% gets the SULT1A1 upregulation without the scalp-flaking penalty.
The two are layered on the same evening application — minoxidil first, then tretinoin after the minoxidil has fully dried (~10 minutes).
Downsides. Scalp irritation, occasional flaking, the cosmetic inconvenience of an oily scalp at bedtime. Some users develop contact dermatitis to propylene glycol (the standard vehicle) — switching to a foam or alcohol-only vehicle resolves this.
Ketoconazole 2% shampoo
The third leg of the topical layer. Antifungal originally for dandruff and seborrheic dermatitis; used in AGA protocols for two reasons.
Mechanism.
- Antifungal. Clears Malassezia overgrowth on the scalp. Malassezia drives a chronic low-grade inflammatory state at the follicle level, and that inflammation accelerates fibrosis. Clearing the fungal load lowers the inflammation tax on the protocol.
- Weak androgen receptor antagonism. Ketoconazole has measurable anti-androgenic activity at the follicle level — not strong enough to be a primary therapy, but useful as a free additive on top of the rest of the stack.5
Dose. Two concentrations are commonly available in Malaysia — both work, with a tradeoff between potency and frequency.
| Concentration | Frequency | Notes |
|---|---|---|
| Ketoconazole 2% | 2–3× per week | The mainstream protocol. Higher potency per use, but more drying. Available OTC in Malaysia under Nizoral and Ketomed. |
| Ketoconazole 1% | 3–5× per week | Standard OTC Nizoral formulation. Gentler per use, can be used more often, comparable cumulative effect. Better tolerated by users with dry or sensitive scalps. |
Application is the same regardless of strength: massage into the scalp, leave for 5–10 minutes, rinse thoroughly. The sit time matters — quick rinses underdose the antifungal effect.
Downsides. Hair texture can feel dry initially; alternating with a normal moisturizing shampoo on off-days handles this. The 2% concentration is more likely to cause flaking — drop to 1% with higher frequency if it becomes an issue.
Alpha-estradiol (Ell-Cranell, Pantostin)
A topical isomer of estradiol — not the same as estrogen in any meaningful endocrine sense. It’s the alpha epimer, which has very weak estrogenic activity but stronger inhibitory activity at the local 5α-reductase enzyme in the scalp.
Mechanism. Localized inhibition of 5α-reductase at the scalp follicle — gets some of the “block DHT” benefit of systemic finasteride/dutasteride, but kept local to the application zone, without the systemic neurosteroid suppression that produces the motivation/mood cost.
Dose. 0.025% is the European-formulary concentration (the dose Ell-Cranell and Pantostin are sold at). Used as a daily fluid topical — 3 mL spread across the scalp, no rinsing.
Downsides. Mild localized estrogenic effects in rare cases (no systemic feminization at this dose). Cosmetically fine — fluid, non-greasy, dries fast.
Tier 2 — The Research Stack
Compounds without legal sourcing routes in Malaysia, sourced through grey-market research-chemical channels, with varying safety data. Not recommendations — transparency about what exists in the broader protocol space.
RU58841
A non-steroidal selective androgen receptor antagonist originally developed by Roussel-Uclaf in the 1990s as a potential acne and AGA therapy.6 Development was abandoned (commercial reasons, not safety findings) and it now exists exclusively as a research chemical.
Mechanism. Binds androgen receptors in the scalp and prevents DHT from binding. Localized when applied topically — the goal is high local concentration with minimal systemic uptake. The substitute for systemic finasteride explained in the deliberate exclusion section above.
Dose. 5% topical solution in an ethanol/propylene glycol vehicle is the operating concentration. Mixed fresh from powder weekly or sourced pre-made from research suppliers. Applied once daily to the target zones, with 15–20 minutes of dry time before any other topical is layered.
Downsides. No completed long-term human safety trials. Theoretical concerns about systemic uptake at high doses or in damaged-skin states. Vehicle adherence matters — wrong PG/ethanol ratio dramatically reduces follicle penetration.
MK-677 (Ibutamoren)
An oral ghrelin mimetic — covered in Fit Series Part 4.0 in the context of GH/IGF-1 elevation. In the hair stack, the role is shaft-quality enhancement.
Mechanism. Elevates growth hormone and IGF-1 over months. IGF-1 thickens the structural keratin layer of the hair shaft, increasing average shaft diameter (KPI 3 in the [attribution map](Part 1.2 - How to Actually Track and Decide#The attribution map which compound drives which KPI)). Does not address androgenic miniaturization — the choking signal from DHT overrides any growth signaling.
Dose. 20 mg/day, taken before bed (rides the natural overnight GH pulse), in 8-week cycles. Not run continuously — long-term elevation of GH/IGF-1 has its own metabolic costs (insulin sensitivity drift, joint swelling, water retention).
Downsides. Appetite increase (useful during a bulk, problematic during a cut), water retention that masks definition, possible elevated fasting glucose over long use. The 8-week cycle window keeps these manageable.
GHK-Cu (copper peptide)
A naturally occurring tripeptide (Gly-His-Lys) bound to copper. Most published research is on topical tissue remodeling (wound healing, skin elasticity), but systemic SubQ administration produces broader regenerative effects.7
Mechanism. Stimulates tissue remodeling at the follicle bulb — reduces peri-follicular fibrosis, enlarges follicle size, supports the dermal papilla. Synergistic with minoxidil because it acts on the same target tissue from a different angle.
Dose. 2 mg subcutaneous injection, every other day (EOD). SubQ rather than topical is a deliberate choice — systemic dosing reaches the follicle bulb at usable concentration regardless of vehicle penetration, and the broader anti-aging and tissue-remodeling effects (skin, joints, recovery) are bonus.
Downsides. Injection requirement (small-gauge insulin needle, low pain). Mild localized injection-site reaction in some users. Pricier per month than topical preparations.
KPV (anti-inflammatory tripeptide)
A tripeptide fragment (Lys-Pro-Val) derived from α-MSH. Primary published use is inflammatory bowel disease, but the anti-inflammatory mechanism is broadly active and useful for scalp cellular stress8.
Mechanism. Inhibits NF-κB signaling at the cellular level → reduces inflammatory cytokine production → lowers the chronic micro-inflammation that accelerates follicular fibrosis. Supports the rest of the stack by keeping the scalp environment calm enough for topicals to absorb cleanly without triggering contact dermatitis.
Dose. 500 mcg subcutaneous, daily is the typical range used alongside GHK-Cu protocols. (Confirm your exact protocol — published research uses doses anywhere from 200–500 mcg/day depending on application.)
Why SubQ and not topical Both GHK-Cu and KPV can be formulated topically and applied to the scalp post-shampoo. The SubQ route is preferred when (a) systemic anti-inflammatory and tissue-remodeling effects are also desired (joints, skin, recovery), and (b) reliable follicle delivery matters more than localized concentration. Topical peptides face the same vehicle-penetration uncertainty that affects minoxidil and RU58841; SubQ bypasses that.
Downsides. Injection requirement. Limited long-term human data. Cost.
Retatrutide — the indirect hair risk
Retatrutide is in the broader protocol for metabolic and body-recomposition reasons (covered in Fit Series Part 4.0). It is not in the hair stack and does not directly help hair. It belongs in this article for the opposite reason: it can hurt hair.
The mechanism. Rapid weight loss from any cause — caloric restriction, GLP-1/GIP agonists, illness, surgery — can trigger telogen effluvium (TE). A large fraction of scalp follicles synchronously shift into telogen in response to the metabolic stress, then shed 2–4 months later. The shed looks dramatic, often dramatic enough to make someone panic-quit a hair protocol that’s actually working9.
The action item. If retatrutide (or any aggressive fat-loss tool) is running alongside the hair stack, keep the rate of fat loss under 1% of bodyweight per week. Above that rate, TE probability climbs sharply. If a shed happens, hold the stack — TE is reversible, follicles re-enter anagen 3–6 months after the metabolic trigger resolves.
Beyond pharmacology — mechanical and environmental protocols
The compound stack is the chemistry layer. Underneath that, the physical environment of the scalp — cellular energy at the mitochondrial level, tissue elasticity, microcirculation, dermal-papilla mechanotransduction — affects how well every compound above actually works. The protocols in this section don’t replace pharmacology. They multiply it.
Three additions, in order of leverage: microneedling, scalp massage, LLLT.
Red light therapy (LLLT)
Mechanism. Photobiomodulation. Wavelengths in the 650–670 nm range penetrate scalp tissue and reach the base of the follicle. The photons are absorbed by cytochrome c oxidase in the follicular mitochondria, which accelerates ATP production. Higher cellular energy shifts resting (telogen) follicles back into active (anagen) growth and supports the existing anagen pool10.
Dose. 15–20 minutes per session, 3–4 times per week. Consistency over duration — more session minutes per week underperforms shorter, more frequent sessions. Form factor is personal preference:
- Helmet (Capillus, iRestore, Theradome) — covers the scalp uniformly without active management. The “set timer and read” option.
- Panel — cheaper, requires positioning the head correctly.
- Comb — cheapest, requires active sweep technique across all target zones.
Downsides. Slow to show on the KPIs (effects compound over 4–6 months of consistent use). Upfront cost ranges from ~RM800 for entry-level combs to RM3,000+ for full-coverage helmets. Cost is one-time, not recurring.
Scalp massage
Mechanism. Two effects, and the smaller one is what most people think it is. The transient blood-flow bump from massage is real but minor. The actual benefit is mechanical stretching of the dermal papilla cells — the stretching stress upregulates genes associated with hair thickness and tissue remodeling11. Over years, it also helps loosen the subcutaneous scalp tension (calcification and fibrosis at the galea aponeurotica level) that physically restricts blood supply in chronic pattern baldness. I then massage my scalp with a silicon scrubber for 1-2 minutes to stimulate blood flow. Blueprint is now fulfilling Rx for hair.
Dose. 4–5 minutes daily, firm pressure — moving the scalp skin over the skull, not just sliding fingers through the hair. Easiest to layer with shampooing in the shower, or outside with a light carrier oil (jojoba, argan).
Downsides. None to speak of beyond the 4–5 minutes. Mild hair pull initially if technique is sloppy — focus on moving skin, not pulling hair.
Microneedling (dermarolling / dermastamping)
The most potent non-pharmacological intervention in the stack. Also the one with the most layering implications for the rest of the protocol.
Mechanism. Controlled micro-injuries trigger a localized wound-healing cascade. The healing response floods the zone with growth factors, drives collagen production, and meaningfully upregulates the Wnt/β-catenin signaling pathway — the same pathway that the experimental peptide PTD-DBM targets and that underlies dermal papilla activation in anagen12. In multiple published trials, microneedling + topical minoxidil outperforms minoxidil alone on density and shaft response.
Dose. 1.0–1.5 mm needle length, once weekly to once every two weeks. Below 1.0 mm doesn’t reach the dermal papilla layer. Above 1.5 mm risks scarring without additional benefit. Dermastamps are easier to control than dermarollers and produce more uniform depth across the target zone — preferred for protocol use.
Downsides and layering implications. This is where the protocol gets careful.
Do not apply RU58841 within 24 hours of microneedling Microneedling opens transcutaneous channels that dramatically increase systemic absorption of anything applied to the scalp for the next 12–24 hours. For minoxidil this is sometimes desirable — the enhanced penetration is part of the synergy and some protocols deliberately apply minoxidil 12–24 hours post-needle to leverage it.
For RU58841 it is the opposite. The entire reason RU58841 is in this stack instead of systemic finasteride is to keep androgen blockade localized to the scalp. Applying RU58841 to a freshly microneedled scalp converts a topical compound into a systemic one — defeating the localization rationale and increasing the side-effect probability accordingly.
The safe play: microneedle on a specific weekly evening (e.g. Sunday). Skip all topicals that night. Resume the full topical schedule 24 hours later. If running the post-microneedle minoxidil variant, hold RU58841 for a full 48 hours post-needle, then resume.
Sourcing tiers
The Malaysian sourcing reality split into two channels.
Channel 1 — Legal: clinic prescription and pharmacy
Compounds in this channel can be obtained with a doctor’s prescription and a registered pharmacy:
- Oral minoxidil — prescribed off-label by dermatologists and increasingly by general practitioners familiar with AGA. Available as compounded tablets from pharmacies that handle compounding (Caring, Watsons specialty branches, hospital pharmacies).
- Topical minoxidil 5% — over-the-counter as Rogaine and generic equivalents. No prescription required.
- Tretinoin 0.025% — prescription cream, available through dermatology clinics. The brand-name Retin-A and generic tretinoin both work.
- Ketoconazole 2% shampoo — over-the-counter as Nizoral, Ketomed, and generics. No prescription required.
Channel 2 — Grey market: research chemical suppliers
Compounds without a legal pathway in Malaysia, sourced through international research chemical and peptide suppliers:
- Alpha-estradiol (Ell-Cranell, Pantostin) — prescription in EU, no Malaysian equivalent. Personal-import via EU pharmacy channels.
- RU58841 — research chemical only, no medical authorization anywhere. Sourced as pre-made solution or raw powder for self-mixing.
- MK-677 — research chemical, sometimes mis-marketed as a supplement. International peptide suppliers.
- GHK-Cu and KPV — research peptides. International peptide compounding suppliers; reconstituted with bacteriostatic water.
On grey-market sourcing Supplier quality varies enormously. Third-party HPLC testing (verification of purity and concentration) is the only honest way to know what's in a vial. The cheaper the supplier, the more likely the actual concentration deviates from the label. The peptide and research-chem community publishes ongoing supplier comparisons; verify before buying, and verify again after a supplier changes batch.
Bloodwork
Two contexts.
For Tier 1 alone. Annual basic panel is fine. Lipid panel (oral minoxidil can occasionally affect cardiovascular markers), kidney function (filtration of the active metabolite), liver panel (ketoconazole shampoo absorption is minimal but worth a periodic check). No special protocol beyond what a yearly physical covers.
For Tier 1 + Tier 2. Integrate with the existing yearly bloodwork pulled for the broader enhancement and biomarker protocols. The hair stack doesn’t require a separate testing cycle — most relevant markers are already being monitored (hormone panel, lipid panel, hematocrit, kidney/liver, HbA1c). Pull the panel pre-cycle and post-cycle for any new compound; otherwise the annual cadence covers the rest.
Cycled compounds (MK-677 ≤ 8 weeks) — don’t chase fluctuations within a cycle. Fasting glucose will drift up while on MK-677; lipids may shift; that’s expected and reverses off-cycle. The reason to keep cycles ≤ 8 weeks is precisely so these transient changes don’t entrench.
When to pull bloodwork outside the annual cadence Three triggers: (1) introducing a new Tier 2 compound — pull baseline before and 4–8 weeks after, (2) a new symptom that could be metabolic (fatigue, swelling, libido shift), (3) any sustained side effect from a Tier 1 compound (ankle swelling, palpitations from oral minoxidil) — confirm with bloodwork rather than self-diagnosing.
The optimized daily and weekly schedule
The schedule below separates conflicting topical vehicles, prevents scalp saturation, and layers the protocol so nothing wastes another compound’s effect.
| Time | Step | Notes |
|---|---|---|
| 8:00 AM | Oral minoxidil + any daily systemics. Topical alpha-estradiol applied to clean, dry scalp. | Alpha-E2 is fluid and non-greasy — won’t disrupt hairstyling for the day. |
| In-shower or evening | Scalp massage 4–5 min, firm pressure. Move skin over skull, don’t pull hair. | Easiest to layer with shampooing or with a light carrier oil. |
| 9:00 PM | Topical RU58841 (5% in ethanol/PG) to target zones. Let dry for 15–20 minutes before any other topical. | Dry time is non-negotiable — wet RU58841 mixed with the next layer’s vehicle reduces receptor binding. |
| 9:30 PM | Topical minoxidil (5%) + tretinoin (0.025%) layered. Minoxidil first, dry ~10 min, then tretinoin. | Tretinoin upregulates SULT1A1 overnight, maximizing the next morning’s minoxidil bioavailability. |
| Mon / Wed / Fri (or 2× weekly if using 2%) | Ketoconazole shampoo wash (1% 3–5× weekly or 2% 2–3× weekly). Massage in, sit 5–10 min, rinse. | Strips vehicle residue (PG buildup), clears sebum-DHT, calms inflammation. |
| 3–4× per week | LLLT 15–20 min (helmet, panel, or comb). | Anytime convenient — watching TV, working, reading. Consistency over duration. |
| Weekly (e.g. Sun PM) | Microneedling 1.0–1.5 mm dermastamp on target zones. | Skip all topicals that night. Resume 24h later (48h for RU58841 if applying post-needle minoxidil). |
| EOD (e.g. Mon / Wed / Fri / Sun) | GHK-Cu 2 mg SubQ injection. | Rotate site (abdomen, thigh, deltoid). Pre-dawn or before-bed timing is convenient. |
| Daily | KPV 500 mcg SubQ injection. | Rotate site. Adjust dose per your specific protocol. |
| 8 weeks on / 4 weeks off | MK-677 20 mg orally before bed. | Cycle duration is the protective mechanism — see Cycle management. |
Layering rules
Four rules govern how the topicals and mechanical interventions interact. Violate them and the stack underperforms — or, in the case of rule 4, becomes actively unsafe.
- Always allow full dry time between conflicting vehicles. RU58841’s ethanol/PG vehicle and minoxidil’s PG vehicle don’t share well when both are wet — mixing concentrations changes absorption profiles. Dry RU58841 (15–20 min) → then minoxidil → dry (10 min) → then tretinoin.
- Ketoconazole washes go on non-application days where possible. If the schedule forces a wash on a topical day, do the wash in the morning or early evening, give the scalp 3–4 hours to recover, then apply the evening topicals.
- Alpha-estradiol is morning-only; the heavy topical stack is evening-only. Splitting the load prevents a single scalp saturation event from overwhelming absorption capacity. Mixing morning and evening topicals into one session reduces total uptake.
- Microneedling pauses the topical schedule. No topicals the night of needling. The full evening topical sequence resumes 24 hours later. If the protocol applies minoxidil at the 24-hour mark to leverage enhanced penetration, RU58841 holds for 48 hours post-needle to avoid systemic uptake. LLLT and scalp massage continue normally — they don’t open transcutaneous channels.
Cycle management
Most of the stack is daily-forever. Two compounds are cycled.
MK-677 — 8 weeks on, 4 weeks off. GH/IGF-1 elevation is useful in pulses, not as a baseline. Continuous use drifts insulin sensitivity, retains water, and increases the side-effect probability without proportional benefit. The 8-week window is enough to drive a measurable shaft-diameter response at the next clinic scan; the 4-week off period normalizes the metabolic markers.
Retatrutide — pulsed for fat-loss phases. Not a daily-forever compound. When running, keep fat loss to <1% bodyweight per week to avoid TE-triggered hair shedding. Off-phases (recomp, maintenance, lean bulk) — the hair stack runs normally without interaction.
Don't cycle the rest RU58841, alpha-estradiol, oral minoxidil, topical minoxidil + tretinoin, ketoconazole, GHK-Cu, KPV — these are protective and rescue compounds. They work by being present at the receptor or follicle every day. Cycling them is just letting the protocol break.
How to think about all of this
The honest hierarchy of impact for hair, from most to least:
- Catching it early enough that follicles are still in state 1 or state 2 — not state 3. No protocol can recover fibrosis. The earliest possible intervention is always the highest-leverage one.
- Daily adherence to the protocol you’re actually running — even a suboptimal stack run consistently outperforms an optimal stack run sporadically.
- Tier 1 compounds (oral minoxidil + topical min/tretinoin + ketoconazole + alpha-E2) — collectively responsible for the majority of measurable density and shaft response.
- Mechanical layer (microneedling, scalp massage, LLLT) — multiplies the chemistry above it. Microneedling specifically has the strongest evidence for synergy with minoxidil. Free relative to compound costs once the equipment is bought.
- Tier 2 compounds (RU58841, MK-677, GHK-Cu, KPV) — meaningful on top of Tier 1 + mechanical; trivial without them.
- Hair transplantation — the only solution for fibrosed zones, and the insurance the stack protects after the fact.
People run this hierarchy backward. They stack RU58841 and MK-677 while skipping topical minoxidil on weekends, never microneedling, and never getting a baseline scan. Get the diagnostic loop running, lock down Tier 1 adherence and the mechanical layer, and only then evaluate whether Tier 2 has anything to add.
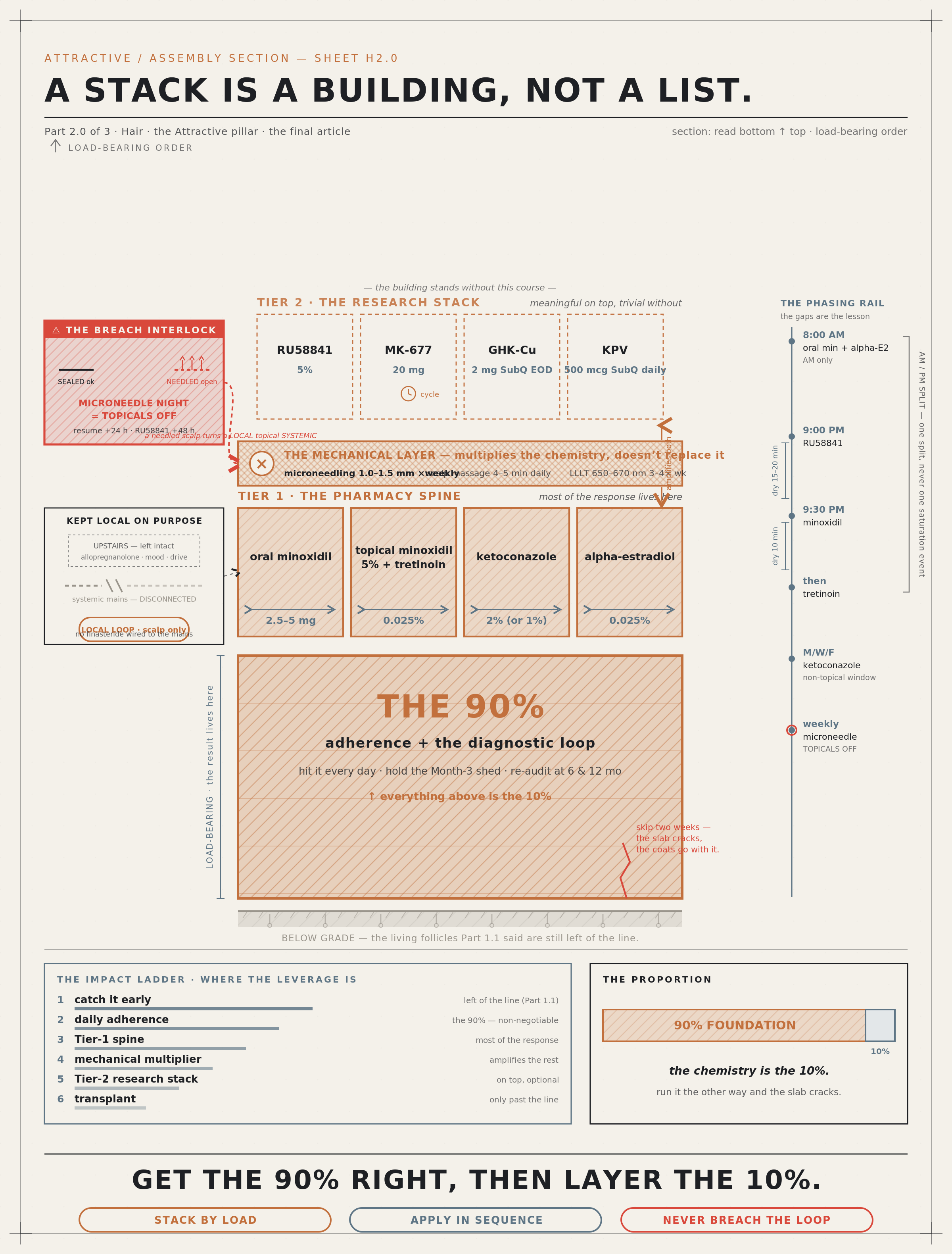
Here’s the whole protocol drawn as one building — because a stack is a building, not a list. A massive 90% foundation of adherence carries a thin 10% of chemistry, built up in load-ordered courses: the Tier-1 pharmacy spine, the mechanical multiplier layer, and the optional Tier-2 top course — read bottom-to-top for what carries what. Down the side, the phasing rail times every coat and dimensions the dry-time gaps, and the single red interlock marks the one rule you can’t break: a needled scalp turns a local topical systemic. Get the 90% right, then layer the 10% — pin it up and re-check the order every week.
Part 2.0 Takeaways
Key concepts to internalize
- The 90/10 rule applies here too. The diagnostic loop and basic adherence produce most of the result. Compound choice is the margin.
- No finasteride or dutasteride — mechanism conflict with DHT-derivative use, and the allopregnanolone/motivation cost isn’t worth the convenience. RU58841 substitutes for the receptor blockade locally.
- Tier 1 is the spine: oral minoxidil 2.5–5 mg, topical minoxidil 5% + tretinoin 0.025%, ketoconazole 2% 3× weekly, alpha-estradiol 0.025% daily. Most of the response lives here.
- Tier 2 layers on top: RU58841 5% topical, MK-677 20 mg on 8-week cycles, GHK-Cu 2 mg SubQ EOD, KPV 500 mcg SubQ daily.
- Retatrutide is a hair risk, not a hair drug. Aggressive fat loss triggers telogen effluvium. Cap loss at <1% bodyweight per week when retatrutide is running.
- Ketoconazole comes in two strengths: 2% (2–3× weekly, more drying) or 1% (3–5× weekly, gentler). Equivalent cumulative effect, pick by scalp tolerance.
- Mechanical interventions multiply pharmacology. Microneedling (1.0–1.5 mm, weekly) is the strongest single addition; daily scalp massage (4–5 min, firm pressure, move skin not hair) and LLLT (15–20 min, 3–4× weekly, 650–670 nm) are additive.
- Microneedling has hard layering rules. Skip all topicals the night of needling. Resume 24 h later. RU58841 specifically holds 48 h post-needle if minoxidil is applied at the 24 h mark — because microneedling converts topical RU58841 into a systemic compound, defeating the localization rationale.
- Sourcing splits cleanly into two channels. Channel 1: prescription/OTC through Malaysian clinics and pharmacies (oral min, topical min, tretinoin, ketoconazole). Channel 2: grey market for everything else.
- Bloodwork rides the existing annual cadence for users already pulling enhancement/biomarker panels. No separate hair bloodwork protocol needed. Cycled compounds (MK-677) don’t need within-cycle monitoring.
- Layering rules matter: dry time between vehicles, morning vs. evening split, ketoconazole on non-topical days where possible, microneedling pauses topicals for 24–48 h.
- Cycle MK-677 and retatrutide; don’t cycle anything else. The rest of the stack works by being present every day at the receptor or follicle.
Your Tier-1 Stack Task List
This is the executable starting point. Tier 2 only after Tier 1 is locked in and the Part 1.2 diagnostic loop is running.
- Book a dermatologist consult for oral minoxidil and tretinoin prescriptions. State you’ve already done the diagnostic baseline (or have it scheduled). Most dermatologists in Malaysia familiar with AGA will prescribe oral minoxidil at 2.5 mg without resistance.
- Source the OTC layer — topical minoxidil 5% (Rogaine or generic), ketoconazole shampoo (Nizoral 1% standard, or 2% prescription/specialty pharmacy). Both available without prescription at major pharmacy chains.
- Source alpha-estradiol via EU personal import if running it. Ell-Cranell and Pantostin are the brand options.
- Acquire the mechanical-layer tools. Dermastamp 1.0–1.5 mm (RM30–RM80 on Shopee/Lazada — buy from a vendor with stainless-steel needles and a sealed package, not cheap titanium-coated knockoffs). LLLT device if budget allows (RM800 entry-level comb → RM3,000+ helmet — helmet is the consistency-friendly choice). Fingers cost zero.
- Set the daily schedule per The optimized daily and weekly schedule. Calendar the 8 AM / 9 PM / 9:30 PM blocks, the ketoconazole wash days, the weekly microneedle slot (and the topical pause around it), and the LLLT sessions.
- Stockpile a 3-month supply of every active before starting. Running out mid-protocol for any compound resets the adherence clock.
- Hold through the Month-3 dread shed — the combined oral minoxidil + topical minoxidil + tretinoin shed is expected and positive. Do not change the stack.
- Re-evaluate at the Month-6 audit per Part 1.2’s decision tree. Tier 2 additions, dose increases, or vehicle changes are considered here — not before.
That's the three-part Hair Series
- Part 1.1 — What Actually Matters — the biology, KPIs, and measurement tiers.
- Part 1.2 — How to Actually Track and Decide — baseline lock-in, clinic strategy, attribution map, 12-month timeline, and the Month-6 decision tree.
- Part 2.0 (this article) — the pharmacology and the daily layered schedule.
The point of writing this wasn’t to provide a copy-paste protocol — it’s to provide the reasoning, so each reader can build their own version that fits their starting follicle state, genetics, risk tolerance, and what they’re willing to source. Take whatever’s useful. Ignore whatever isn’t.
Disclaimer This article describes pharmacological compounds and grey-market research chemicals that are not approved as hair-loss treatments in most jurisdictions and that carry varying health risk profiles if used without medical supervision. Nothing here is medical advice or a recommendation to use any specific compound.
Anyone considering Tier 2 compounds should work with a qualified physician familiar with research-chemical pharmacology, pull comprehensive bloodwork, and understand the long-term risk profile of what they’re putting on their scalp and into their body. The grey-market portion of this stack has limited long-term human safety data; this is shared for transparency, not endorsement.
Sources & references
Footnotes
-
5α-reductase converts progesterone to allopregnanolone, a positive allosteric modulator of GABA-A receptors. See PubMed Central — PMC2670437 on allopregnanolone neurosteroid pharmacology; review at Wikipedia — Allopregnanolone. ↩
-
Post-finasteride syndrome and allopregnanolone reduction: Giatti et al. (2018), “Post-finasteride syndrome and post-SSRI sexual dysfunction: two sides of the same coin?” Endocrine. See also PubMed — post-finasteride syndrome for the broader literature. ↩
-
Low-dose oral minoxidil for AGA: see Randolph & Tosti (2021), “Oral minoxidil treatment for hair loss: A review of efficacy and safety,” J Am Acad Dermatol; comprehensive overview at PubMed — low-dose oral minoxidil AGA. ↩
-
Sulfotransferase (SULT1A1) and minoxidil bioactivation; tretinoin upregulation of SULT1A1: Goren et al. (2014), “Clinical utility and validity of minoxidil response testing in androgenetic alopecia,” Dermatol Ther. ↩
-
Ketoconazole anti-androgenic activity at the follicle level: Piérard-Franchimont et al. (1998), “Ketoconazole shampoo: effect of long-term use in androgenic alopecia,” Dermatology. Mechanism review at PubMed — ketoconazole alopecia. ↩
-
RU58841 mechanism and original development: Battmann et al. (1994), “RU58841, a new specific topical antiandrogen: a candidate of choice for the treatment of acne, androgenetic alopecia and hirsutism,” J Steroid Biochem Mol Biol. Receptor-binding studies from the Roussel-Uclaf development program. ↩
-
GHK-Cu tissue remodeling and follicle effects: Pickart et al. (2015), “The human tripeptide GHK-Cu in prevention of oxidative stress and degenerative conditions of aging,” Biomed Res Int. See PubMed Central — PMC4488527. ↩
-
KPV anti-inflammatory mechanism (NF-κB inhibition): Dalmasso et al. (2008), “PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation,” Gastroenterology. Mechanism overview at PubMed — KPV anti-inflammatory. ↩
-
Telogen effluvium triggered by rapid weight loss: American Academy of Dermatology — telogen effluvium; Headington (1993), “Telogen effluvium: new concepts and review,” Arch Dermatol. Specific to GLP-1/GIP agonist-induced TE: emerging case-series literature, e.g., Choi et al. (2024) on semaglutide-associated hair shedding. ↩
-
Low-level laser therapy (LLLT) for AGA, photobiomodulation mechanism, optimal 650–670 nm wavelength: Avci et al. (2014), “Low-level laser (light) therapy (LLLT) for treatment of hair loss,” Lasers Surg Med; meta-analysis at PubMed — LLLT androgenetic alopecia. FDA-cleared devices (HairMax, Capillus, iRestore, Theradome) operate in this range. ↩
-
Scalp massage and dermal papilla mechanotransduction: Koyama et al. (2016), “Standardized scalp massage results in increased hair thickness by inducing stretching forces to dermal papilla cells in the subcutaneous tissue,” ePlasty. Mechanism review on mechanical stress and follicle gene expression. ↩
-
Microneedling for AGA and Wnt/β-catenin pathway activation: Dhurat et al. (2013), “A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: a pilot study,” Int J Trichology — the foundational trial showing microneedling + minoxidil outperforms minoxidil alone. Mechanism review at PubMed — microneedling androgenetic alopecia. ↩